
Source: The paradigm was originally developed in 1978 by Gerben DeJong, now with the National Rehabilitation Hospital in Washington, D.C. It has been modified since then by Maggie Shreve, an organization development consultant working in the field of disability rights out of Chicago, and Steve Brown, a disability policy consultant and principle co-owner of the Institute for Disability Culture in Santa Fe, New Mexico.
The graphic compares the medical model of disability and the Independent Living paradigm of disability. An accessible table is provided below the image.
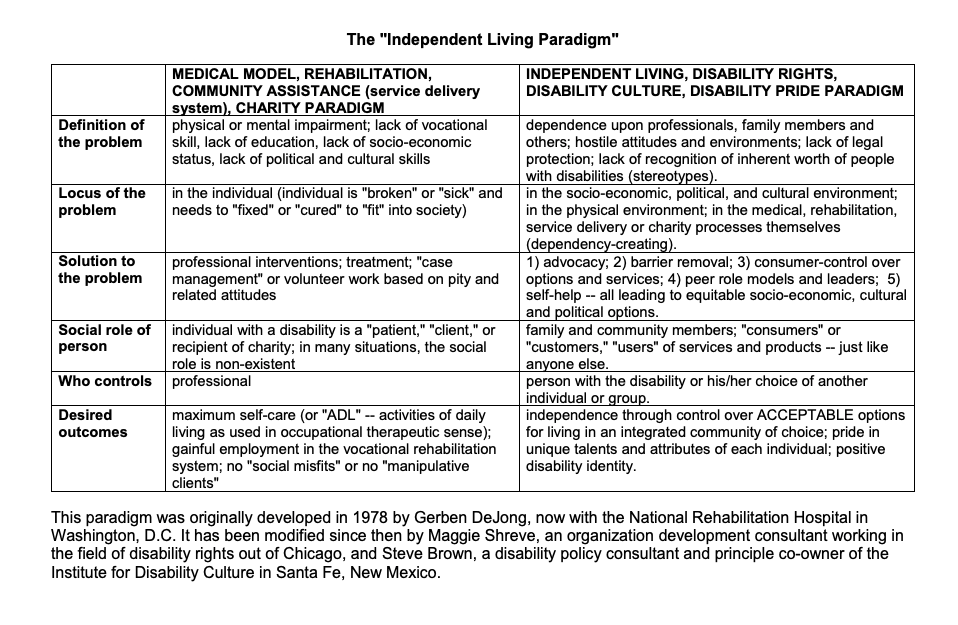
Medical Model, Rehabilitation Community Assistance (service delievery System), Charity Paradigm
Definition of the problem: physical or mental impairment; lack of vocational skill, lack of education, lack of socio-economic status, lack of political and cultural skills
Locus of the problem: in the individual (individual is “broken” or “sick” and needs to “fixed” or “cured” to “fit” into society).
Solution to the problem: professional interventions; treatment; “case management” or volunteer work based on pity and related attitudes.
Social Role of person: individual with a disability is a “patient,” “client,” or recipient of charity; in many situations, the social role is non-existent.
Who controls: professional
Desired outcomes: maximum self-care (or “ADL” – activities of daily living as used in occupational therapeutic sense); gainful employment in the vocational rehabilitation system; no “social misfits” or no “manipulative clients”
Independent Living, Disability Rights, Disability Culture, Disability Pride Paradigm
Definition of the problem: dependence upon professionals, family members and others; hostile attitudes and environments; lack of legal protections; lack of recognition of inherent worth of people with disabilties (stereotypes).
Locus of the Problem: in the socio-economic, political, and cultural environment; in the physical environment; in the medical, rehabilitation, service delievery or charity processes themselves (dependency-creating).
Solution to the problem: 1) advocacy; 2) barrier removal; 3) consumer control over options and services; 4) peer role models and leaders; 5) self-help- all leading to equitable socio-economic, cultural and political options.
Special role of person: family and community members; “consumers” or “customers,” “user” of services and products- just like anyone else.
Who controls: person with the disability or his/her choice of another individual or group.
Desired outcomes: independence through control over ACCEPTABLE options for living in an integrated community of choice; pride in unique talents and attributes of each individual; positive disability identity.